A peptide protocol is a structured, physician-supervised plan that specifies which peptide compound to use, at what dose, by which delivery method, and for how long, in order to achieve a defined health outcome. Knowing how to choose peptide protocols correctly starts with one question: what is your primary, measurable goal? Whether you are targeting weight management with GLP-1 agonists like semaglutide, tissue recovery with BPC-157, or growth hormone support with CJC-1295/Ipamorelin, the selection process follows the same evidence-tiered framework. This article walks you through every decision point, from goal definition and administration route to baseline labs and protocol evaluation.
How to choose peptide protocols based on your primary goal
The single most important rule in selecting peptide protocols is to define one primary goal before choosing any compound. Trying to address weight loss, recovery, and anti-aging simultaneously in a first cycle produces no usable baseline. You cannot tell which peptide is working, which is causing side effects, or what to adjust.
The four most common goals and their best-supported peptide categories break down as follows:
- Weight management: GLP-1/GIP receptor agonists such as semaglutide and tirzepatide carry the strongest evidence tier. GLP-1 peptides are FDA-approved with randomized controlled trial data, making them the default first choice for metabolic goals.
- Tissue recovery: BPC-157 (Body Protection Compound 157) shows consistent results in preclinical models for tendon, muscle, and gut repair. Human trial data is still accumulating, placing it in the clinical/investigational tier.
- Growth hormone support and anti-aging: CJC-1295 combined with Ipamorelin stimulates natural GH secretion. This combination sits in the physician-compounded tier with growing clinical use but lacks large-scale RCT data.
- Cognitive support: Semax and Selank are nootropic peptides with Eastern European clinical data but limited Western regulatory review. They belong in the investigational tier for most U.S.-based protocols.
Evidence quality dramatically influences risk-benefit balance. Prioritize FDA-approved or late-stage clinical peptides before moving to investigational anti-aging options. This is not about being conservative for its own sake. It is about having a safety net when something unexpected happens.
Pro Tip: Start with the peptide that has the most accessible monitoring and the clearest regulatory status. A well-monitored GLP-1 protocol will teach you more about your metabolic response in 12 weeks than a poorly tracked stack of five investigational compounds ever will.
What administration route is right for your protocol?
Route of administration impacts absorption, onset timing, and the practical demands placed on you as the patient. Matching the delivery method to both the peptide's chemistry and your comfort level is a core part of choosing peptide therapy correctly.
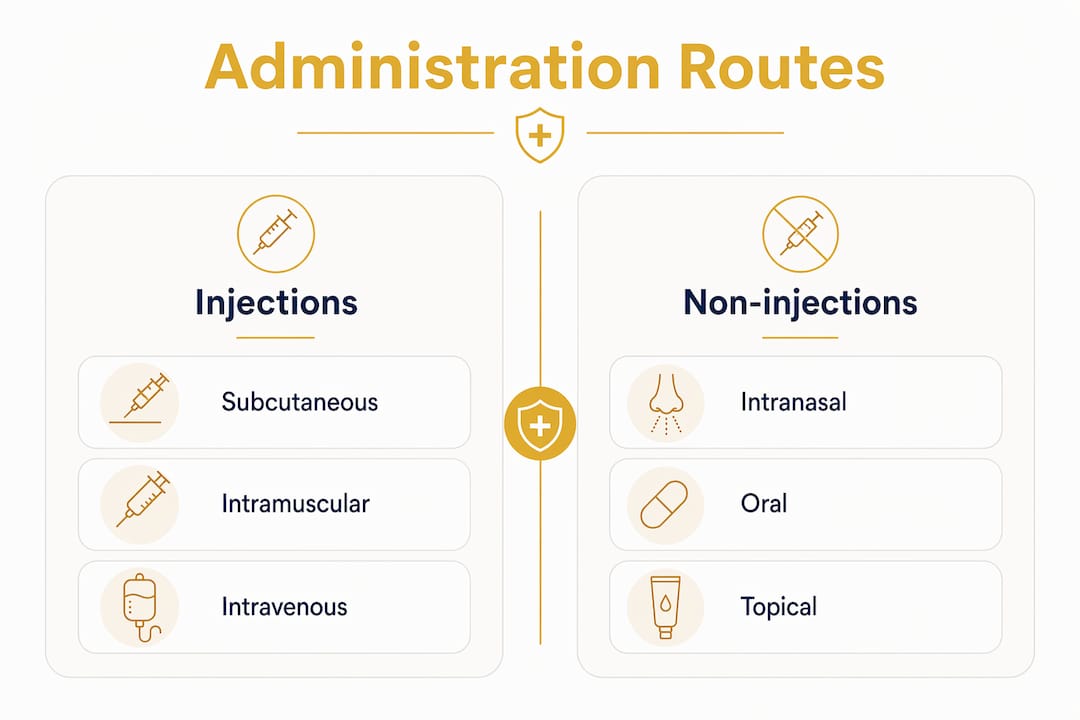
| Route | Bioavailability | Ease of use | Best for |
|---|---|---|---|
| Subcutaneous injection | High (near 100%) | Moderate (requires reconstitution or prefilled pen) | GLP-1 agonists, CJC-1295/Ipamorelin, BPC-157 |
| Intranasal | Moderate (varies by peptide) | High (no needles) | Semax, Selank, PT-141 |
| Oral | Very low (1 to 2%) | High (familiar format) | Limited peptides; mostly research context |
| Topical | Low to moderate | High | Localized applications only |
Injectable peptides degrade rapidly in the gastrointestinal tract, which is why oral bioavailability can fall as low as 1 to 2%. For any peptide where therapeutic dose precision matters, subcutaneous injection is the standard. Intranasal delivery works well for cognitive peptides like Semax, where the olfactory pathway allows direct CNS access and avoids GI degradation.
Dose ranges for common protocols give you a practical starting point. BPC-157 is typically dosed at 250 to 500 mcg per day subcutaneously. CJC-1295 with Ipamorelin is commonly used at 100 mcg of each, administered before sleep to align with natural GH pulses. Semax intranasal doses start at 200 to 600 mcg per day. These are starting ranges, not fixed prescriptions. Your provider adjusts based on labs and response.
Pro Tip: If needle anxiety is a real barrier for you, start with an intranasal peptide or a prefilled GLP-1 pen. Adherence is the most underrated variable in any protocol. A peptide you actually use consistently beats a theoretically superior one you skip.
Why baseline testing is non-negotiable before starting
Baseline labs are the foundation of any safe peptide protocol. Without them, you have no reference point to detect metabolic changes, no data to guide dose adjustments, and no way to prove the protocol is working. The minimum panel before starting any peptide therapy includes:
- CBC (Complete Blood Count): Screens for anemia, immune abnormalities, and platelet issues.
- CMP (Comprehensive Metabolic Panel): Assesses kidney function, liver enzymes, electrolytes, and blood glucose.
- IGF-1 (Insulin-like Growth Factor 1): Required before starting any GH-axis peptide such as CJC-1295/Ipamorelin. Elevated IGF-1 is associated with increased cancer risk and insulin resistance.
- Glucose and HbA1c: Mandatory for GLP-1 protocols and any metabolic health goal.
- Fasting insulin: Useful for anyone with weight management goals to establish metabolic baseline.
Safety monitoring for GH secretagogues requires a follow-up consult at 4 to 6 weeks and an IGF-1 retest at 8 to 12 weeks. This timeline exists because metabolic changes from GH-axis peptides can occur silently. You will not feel supraphysiological IGF-1 levels until the problem is already significant.
Red flag: Any provider who starts you on a peptide protocol without a predefined monitoring schedule is operating outside safe clinical practice. If your clinic does not offer baseline labs, self-order them through services like LabCorp or Quest Diagnostics before your first dose.
Providers without a monitoring plan represent a genuine safety gap. Patients in that situation lose clinical oversight at the exact moment they need it most. Document your own symptom scores weekly using a simple 1 to 10 scale for energy, sleep quality, recovery, and any side effects. This log becomes your evidence base at the 8-week reassessment.
Pro Tip: Set a calendar reminder for your 8-week lab retest on the same day you start your protocol. Waiting until you "feel ready" means most people never retest at all.
Step-by-step guide to setting up your first peptide protocol cycle
A structured workflow removes guesswork and protects you from the most common mistakes in peptide therapy protocols.
- Define one measurable goal. "Lose 15 pounds in 16 weeks" is measurable. "Feel better" is not. Your goal determines your peptide category and your success criteria.
- Get baseline labs. Order CBC, CMP, and goal-specific markers (IGF-1 for GH peptides, HbA1c for metabolic protocols) before your first dose. Review results with a licensed provider.
- Select a provider with oversight. Choose a physician-supervised platform that uses compounded peptides from licensed U.S. pharmacies. FDA-approved and physician-compounded peptides have quality and regulatory oversight that research-grade peptides sold "for research only" simply do not.
- Start at a conservative dose. Begin at the lower end of the therapeutic range and hold that dose for at least two weeks before any adjustment. Your body's response in weeks one and two tells you more than any theoretical dosing chart.
- Schedule dosing consistently. GH-axis peptides work best administered before sleep. GLP-1 agonists follow weekly injection schedules. Consistency in timing improves both efficacy and side effect predictability.
- Track weekly. Log energy, sleep, body composition changes, injection site reactions, and any unusual symptoms. A simple spreadsheet works. The goal is data, not perfection.
- Reassess at 8 to 12 weeks. First protocol cycles require a minimum of 8 weeks to evaluate measurable benefits safely. At that point, review labs and symptom logs with your provider. Then decide: adjust dose, continue as-is, switch peptides, or add a second compound.
The most common mistakes in first cycles are stacking multiple peptides before establishing a baseline, skipping the 8-week lab retest, and sourcing peptides without regulatory oversight. Each of these errors makes it impossible to know what is actually happening in your body.
Pro Tip: Treat your first cycle as a controlled experiment, not a transformation program. The data you collect in cycle one is what makes cycle two genuinely effective.
How to troubleshoot when your protocol is not working
Most protocol problems fall into four categories, and each has a specific fix.
- No noticeable benefit after 6 weeks: Check adherence first. Missed doses, inconsistent timing, and improper reconstitution are the most common culprits before blaming the peptide itself. Then review your dose relative to your body weight and goal.
- Side effects that persist beyond two weeks: Injection site reactions, water retention, and mild fatigue are common in the first two weeks of GH-axis protocols. Persistent or worsening symptoms require a provider consult and a lab check, not a dose increase.
- Cost and sustainability: GLP-1 agonists from compounding pharmacies are significantly more affordable than branded versions. Confirm your provider sources from a licensed U.S. compounding pharmacy to balance cost with quality assurance.
- Needle anxiety: Switch to an intranasal peptide or a prefilled auto-injector pen. For peptide therapy beginners, the psychological barrier of self-injection is real and worth addressing directly rather than pushing through.
- Lab abnormalities: An IGF-1 above 300 ng/mL or a meaningful rise in fasting glucose requires criteria-based dose adjustment. Pre-defining these thresholds before you start means you act on data rather than guessing when a number looks "too high."
Sustainable protocols are built on documentation and honest provider communication. If your provider is not reviewing your symptom logs and lab trends at each follow-up, find one who will.
Key takeaways
Selecting the right peptide protocol requires one defined goal, evidence-tiered peptide selection, a baseline lab panel, and a structured 8 to 12 week evaluation cycle before any stacking or dose escalation.
| Point | Details |
|---|---|
| Start with one goal | Define a single measurable outcome before selecting any peptide compound. |
| Match evidence to risk tolerance | Prioritize FDA-approved GLP-1 agonists or physician-compounded GH peptides before investigational options. |
| Get baseline labs first | CBC, CMP, IGF-1, and glucose markers are required before the first dose. |
| Choose the right delivery route | Subcutaneous injection offers the highest bioavailability; intranasal works for needle-averse users. |
| Evaluate at 8 to 12 weeks | Retest labs and review symptom logs before adjusting dose or adding a second peptide. |
Why I think most people approach peptide protocols backwards
Most people I see researching peptide therapy arrive with a stack already in mind. They have read about BPC-157, CJC-1295, and TB-500 in the same forum thread and want all three at once. The goal is vague, the monitoring plan is nonexistent, and the source is a gray-market website with no pharmacy oversight.
The uncomfortable truth is that peptide therapy without lab monitoring is not health optimization. It is guesswork with a needle. I have seen protocols where the only feedback loop was "I feel pretty good," and those are the same protocols that produce surprises at the annual physical. Supraphysiological IGF-1 does not announce itself. Neither does early insulin resistance from a poorly managed metabolic protocol.
What actually works is the boring version: one goal, one peptide, baseline labs, consistent dosing, and an honest reassessment at week eight. The people who follow that structure are the ones who build genuinely effective long-term protocols. They also have the data to have real conversations with their providers rather than just hoping the next compound will be the one that finally works.
The evidence in peptide therapy is evolving fast, and cautious optimism is the right posture. Some investigational peptides will earn their place in mainstream protocols over the next decade. But right now, the best thing you can do is build a foundation of monitored, evidence-supported cycles before you explore the frontier compounds. Patience and data beat enthusiasm every time.
— Roosevelt
Start your peptide protocol with expert guidance from Grownupmeds
Grownupmeds takes the guesswork out of peptide therapy by connecting you with licensed physicians who design protocols around your specific health goals, not generic templates.
Every Grownupmeds protocol begins with a physician-supervised health assessment, baseline lab review, and a monitoring plan built in from day one. Peptides are sourced exclusively from licensed U.S. compounding pharmacies, so you get the regulatory oversight and quality assurance that research-grade sources cannot provide. Whether your goal is weight management, recovery, or anti-aging support, the clinical team at Grownupmeds provides ongoing follow-up and dose adjustment guidance throughout your cycle. Explore peptide therapy options at Grownupmeds and start with a protocol designed to produce measurable results safely.
FAQ
What is a peptide protocol?
A peptide protocol is a physician-supervised plan specifying a peptide compound, dose, delivery method, and treatment duration aligned to a defined health goal. It always includes a monitoring schedule with baseline and follow-up lab work.
How long should a first peptide protocol cycle last?
First cycles are planned for a minimum of 8 to 12 weeks, including baseline bloodwork review before any dose adjustment or continuation decision is made.
Which peptides have the strongest evidence for weight loss?
GLP-1 receptor agonists such as semaglutide carry FDA approval and randomized controlled trial support, making them the highest-evidence option for weight management peptide protocols.
Do I need labs before starting peptide therapy?
Yes. CBC, CMP, and goal-specific markers such as IGF-1 for GH-axis peptides or HbA1c for metabolic protocols are required before the first dose to establish a safe baseline.
Can I use multiple peptides at once?
Stacking multiple peptides is not recommended in a first cycle. Starting with one peptide creates a usable baseline so you can identify what is working, what is causing side effects, and what to adjust before adding a second compound.